There are three goals for PAD treatments:
- Reducing cardiovascular risk
- Preventing lower limb loss
- Restoring walking capacity and improving quality of life
To control the narrowing of blood vessels due to buildup of fatty deposits, you are encouraged to undergo:
- Regular screening of risk factors, i.e. diabetes and cholesterol screening
- Change of lifestyle - quit smoking, low cholesterol diet, moderate exercise, weight reduction
- Taking anti-platelet agents - long term anti-platelet agents (eg. aspirin, plavix, ticlid) reduce the risk of all cardiovascular disease
- Taking statins (e.g. simvastatin, atorvastatin, rosuvastatin or crestor) - to reduce fat deposits in the arteries.
Non-surgical treatment of PAD includes:
- Walking exercise - regular walking exercise of at least 50 minutes, three or more times per week, can help most people with intermittent pain or discomfort when undergoing physical activity due to lack of blood flow, also known as claudication.
- Medication to reduce intermittent claudication symptoms are also available.
These non-surgical treatments are only applicable for certain inpatients with significant symptoms, with the aim to improve the blood supply to the affected tissues. However, if an ulcer or gangrene has already been set in, surgical debridement (removal of dead, damaged, or infected tissue to promote healing) will be needed.
Surgical treatment of PAD includes:
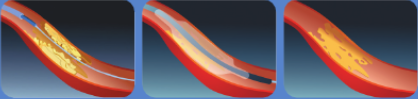
1. Minimally Invasive Endovascular Intervention
The narrowed arteries can be opened using various equipment including guidewires, angioplasty balloons, atherectomy catheters, and stents under X-ray. The procedure will be carried out through a puncture over the groin region under local or regional anaesthesia.
2. Arterial Bypass Surgery
A bypass can be made between the unobstructed arteries, also known as patent arteries, above and below the site of obstruction. Surgical Incisions are needed to expose the arteries for bypass. Either the patient's own vein or a synthetic bypass graft can be used as the bypass conduit.

3. Combination of Endovascular Intervention and Arterial Bypass Surgery
This combination of both endovascular and open bypass treatment is used to treat patients with more complicated arterial occlusive disease.
4. Endarterectomy
In special situations where only a short segment of artery is affected by atherosclerotic plaque, an incision can be made over the vessel for the removal of plaque to improve blood flow through the artery.
5. Minor Amputation and Wound Debridement
If an ulcer or gangrene of the toe and foot has already been set in, minor amputation or wound debridement may be necessary to ensure rapid recovery, and also to restore the walking ability of the individual.
The need for this surgery depends on the location and severity of tissue loss as advised by your specialist.
6. Multi-disciplinary Approach
Besides vascular specialists, we provide a comprehensive care to PAD patients by collaborating with:
- Physicians
- Endocrinologists
- Anaesthetists
- Podiatrists
- Wound-care nursing specialists
- Rehabilitation specialists
With proper treatment and care, the majority of PAD patients with tissue loss are able to heal from their limb ulcer or gangrene, avoid limb loss, and be able to walk again.





.jpg?sfvrsn=62cd560d_1)


