Catheter Ablation
2025/06/03
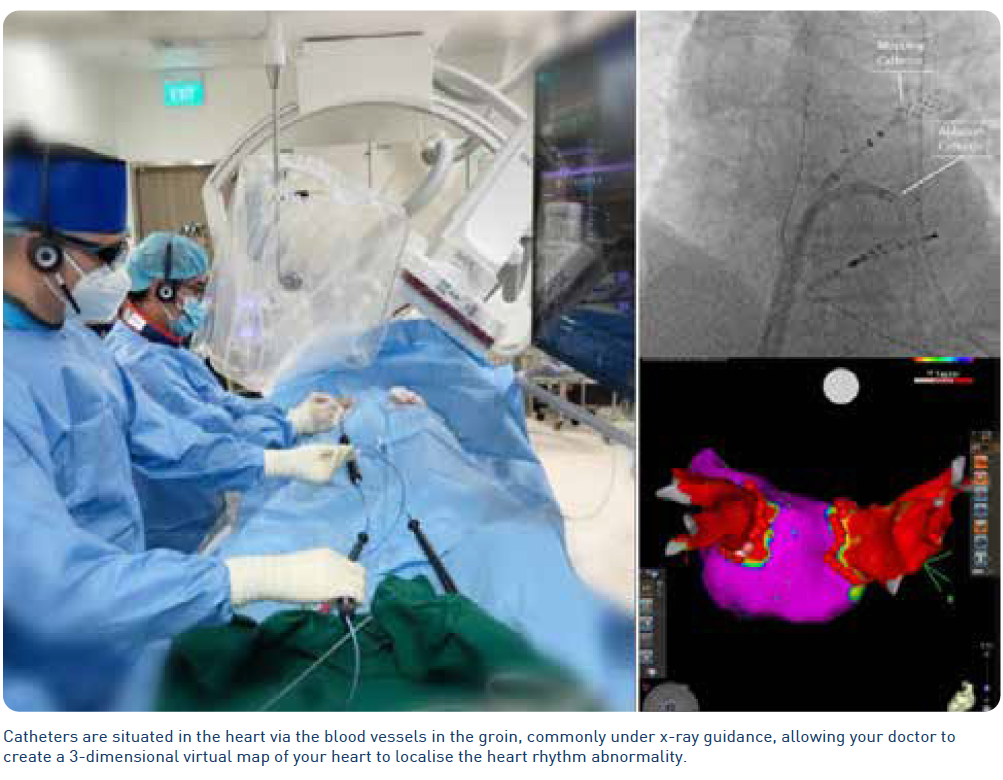
A catheter ablation is a “key-hole” or minimally-invasive procedure on the heart to stop Atrial Fibrillation (AF)/Atrial Tachycardia (AT). This is performed by passing thin, flexible wires called catheters through veins (commonly at the groin level) leading to your heart. Using these catheters, the doctor identifies the origin of abnormal electrical signals causing the heart rhythm disorder.
Small areas of the heart muscle are then modified so that it no longer transmits these abnormal electrical signals. This can be achieved through the application of heat (radio frequency ablation), freezing (cryo-ablation) or an electrical current (pulse field ablation) via the catheter tip.
A catheter ablation may be considered for those who remain significantly symptomatic (e.g. palpitations, effort intolerance, fatigue etc.) from AF/AT despite medications, or for those who are intolerant of medications used to control the heart rhythm. It can also be considered in patients with symptoms who do not wish to take medications on a long term basis. In cases where AF/AT is thought to adversely affect the heart function, an ablation may also be considered.
The procedure is used primarily used to reduce symptoms and improve the quality of life. A successful procedure may also result in reducing or stopping your medications used to regulate your heart rate and rhythm.
Success rates for ablation of an AT are approximately 90%, and up to 80% for paroxysmal AF. In cases of AF, a repeated ablation may be needed to achieve longer-term control. In certain cases of AF, depending on its chronicity and other pre-morbid factors, overall success rates may be a lot lower. Your doctor will advise you of this when an ablation is being considered in such cases.
It is important to note that a catheter ablation is not an alternative to long term blood thinning medications in the prevention of stroke.
- Your doctor will discuss the goals, risks and alternatives of the procedure with you and you will be required to sign a consent form once you are agreeable with the procedure.
- Inform your doctor about any allergies to medications, particularly any reactions to X-ray contrast or heart rhythm medications, as well as any pain-relieving medications you are currently taking.
Follow your doctor’s instructions regarding medications. Your doctor may advise you to stop certain medications before your procedure. - You will most likely be advised to fast from midnight the day before the procedure. If your procedure is scheduled in the afternoon or later in the day, NUHCS staff will advise you a few days before the procedure date on the fasting start time.
- Admission is on the day of the procedure. Do prepare and pack for up to a 2-day stay after the procedure, though in most cases, you may be discharged the next day.
- Preparatory blood tests and an Electrocardiogram (ECG) will need to be performed on the day of admission if they have not been conducted within a month before the procedure.
- If you are undergoing general anaesthesia, a member of the team will perform further assessments prior or on the day of the procedure.
- For women of childbearing age, a pregnancy test may be conducted.
- Pregnant women should not undergo this procedure due to the exposure of X-ray radiation.
- Just before the procedure, your groin and chest may be shaved.
The procedure is performed with your doctor(s) by your side during the entire case with support from the Electophysiology team outside and inside the laboratory.
- An ablation for AF/AT typically takes up to 1 to 2 hours. Procedures performed under general anaesthesia can take up to 3 to 4 hours.
- Your doctor may arrange for a Transoesophageal Echocardiogram (TEE) - an ultrasound scan that has a tube down your swallowing pipe to access the heart. This is to ensure that there are no blood clots within your heart, allowing one to safely proceed with the procedure.
- You will receive medication through an Intravenous (IV) plug to induce relaxation or sleep. If general anaesthesia is used, a plastic tube will be inserted into your windpipe to protect your airway. Under local anaesthesia, you will receive a small injection at the groin, similar to a pinprick.
- The catheters will then be introduced through the groin and positioned within the heart chambers. Electrical measurements and treatment will then be performed via the catheters.
- After treatment, the catheters will be removed and the puncture site wounds will be compressed for a few minutes to stop any bleeding. These wounds should heal within a few days.
- You will need to lie in bed for about 4-8 hours.
- Refrain from moving the limbs where the leads were inserted, so that the blood vessels can heal better and to avoid bleeding.
- If you feel pain or swelling at the insertion (wound) site, please inform the nurse. Painkillers will be prescribed if necessary.
- You should be able to go home the next day.
- Medical leave may be issued so that you can rest at home for a couple of days. You should be able to resume most of your usual activities on the day after discharge.
- Cover the puncture wounds with waterproof plaster for two days, then remove the plaster. Afterward, leave the wound exposed.
Although an ablation for AF/AT is is considered a relatively safe ‘keyhole’ procedure, complications can still occur. These may include pain, swelling, bruising and bleeding from the puncture sites (approximately 5% of all cases). Occasionally, the procedure itself may induce the occurrence of an abnormal heart rhythm that may require an electric shock to terminate. More serious complications, such as strokes, damage to the gullet, heart attacks and damage to the heart or surrounding structures that may require further surgery to correct, are rare (<1% of all cases). In the event of complications, you may need to stay in the hospital for a few more days.
