Paediatric Intensive Care Unit (PICU)
Upon arrival at the PICU, you will be oriented around the ward by a Patient Service Associate to familiarise with the environment. The doctors, nurses and therapists will monitor your child closely to provide the utmost care. You may need to wait outside the ward upon arrival at the PICU as your child needs to be stabilised after returning from the operating theatre.
Please wash your hands or use the antiseptic handrub, which is placed around the ward, before and after visiting your child.
Parents/caregivers can visit their child in the ward at any time. No more than two people are allowed to be at the bedside at any one time.
While your child is in the PICU, your doctor may refer you to the Ronald McDonald House (RMH) or the Ronald McDonald Family Room (RMFR) which provides a place of respite while allowing you to be steps away from your hospitalised child at no cost.
Alternatively, you may choose to return home while your child is sedated. Your health is also important during your child’s recovery process; it is crucial that you receive adequate rest so that you can be there foryour child when he/she is awake. Our doctors and nurses will keep you updated, and you are welcome to return to the ward at any time.
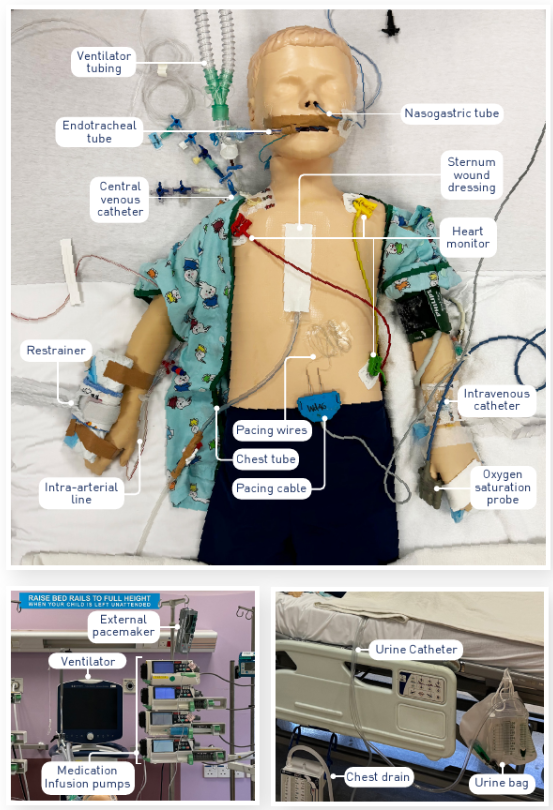
Monitoring and equipment
Monitors - Your child will have stickers and leads attached to them, this is to monitor body functions such as blood pressure, oxygenation level, heart rate, etc
Ventilator - Your child will be on a breathing tube via the nose or mouth, connected to a ventilator to support their breathing. To prevent the tube from being blocked, the nurse will regularly pass another small catheter through the ventilator tube to clear the mucus by suctioning. Chest physiotherapy will also be done to aid in relieving the mucus.
Hand splints and restrainers - Used to keep the hand straight and prevent your child from accidentally pulling or dislodging tubes and lines, an action which could be detrimental to your child’s treatment process.
Nasogastric tube - A tube which is passed through the nostril, down the back of the throat into the stomach. This is to drain stomach fluids and gas to prevent bloating and reduce the chance of vomiting. Medications and milk will also be fed through the tube, and it will be removed once your child is strong enough to feed orally.
Intra-arterial line - A cannula will be inserted in the artery (either from the wrist or groin) for blood pressure monitoring and taking of blood samples for various blood tests to monitor your child’s progress.
Central Venous Catheter (CVC) - An intravenous cannula/line inserted into the large vein on one side of the neck or groin, to aid in administering fluids and medications through it. Blood samples will also be taken for certain blood tests.
Chest drains - During surgery, chest drain(s) will be inserted to drain any blood, fluid or air from the chest cavity. They will also be connected to a container which will gently pull the fluids out. The chest drains will be removed within several days or weeks when appropriate.
Pacing wires -
- Many children will have pacing wires inserted during open-heart surgery. The beating of the heart may be interrupted or slowed down after surgery, and your child will be attached to an external pacemaker, if affected.
- This is to keep the heart beat at the normal rhythm until the heart recovers.
Peritoneal drain - Some children may have reduced kidney function after cardiac surgery. A tube will be inserted into the abdomen to drain unwanted fluids that are collected there.
Urine catheter - A catheter will be inserted to drain and accurately measure urine output for monitoring of fluid status.
Chest X-ray - There will be regular chest x-rays to check the condition of the heart and lungs.
Electrocardiogram (ECG) - Sensors will be attached to the skin to check the heart’s rhythm and electrical activity.
Medications
- Your child will be on continuous infusions that include sedatives and pain relief medication, as well as those that support the heart and blood pressure.
- These medications will gradually be weaned off as your child’s condition improves.
There are also other ways of pain relief: Distracting your child with their favourite TV shows or by playing their favourite music. Holding a folded towel to their chest helps with the discomfort when they cough.
Physiotherapy
- After undergoing heart surgery and anaesthesia, it is common for children to have increased phlegm in their lungs.
- They may be less active than usual, and unable to cough effectively to clear their phlegm, thus often requiring physiotherapy to prevent and reduce the risk of lung infection.
A Physiotherapist will also review your childafter heart surgery:
- For infants: developmental screening and education on various kinds of exercises you can do for your child.
- For toddlers and above: assist in sitting out of bed and going for a walk. Support will be provided for children with mobility issues or chest concerns.
Wound care
- During surgery, the surgeons will use dissolvable stitches to close up the chest wound.
- However, there may be visible stitches on the surface of the skin where the chest drains were placed and these will be removed 10-14 days after surgery in conjunction with your child’s follow-up appointment in the clinic.
