On the first Post-Operative Day (POD), a physiotherapist will be assisting you with mobilization and deep breathing exercises.
There will be a chest drain coming out from you to drain the remaining fluid and air within your chest. This will be connected to a box which the doctor will check daily to determine your progress and recovery. Once it is safe, the chest drain may be removed on POD Day 1 – 3.
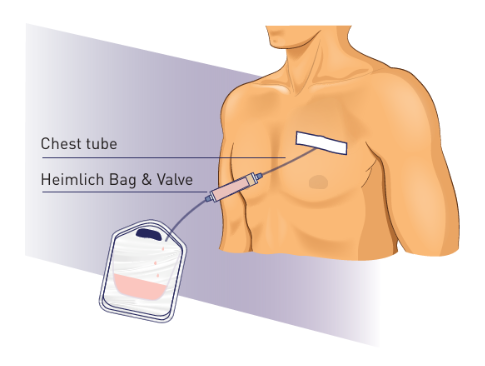
In some cases when you have persistent air leak after surgery, the chest drain may be kept and connected to a one-way valve called a Heimlich bag. Caregiver training will be provided upon discharge and you will be reviewed in the clinic weekly to assess the removal of the drain.
After your chest drain is removed, please follow the discharge post-op care listed below:
1. Wound care
- Shower with mild soap and water
- Ensure surgical wound is thoroughly rinsed
- Dab wound dry with a towel first and then tissue paper
- Do not rub or scratch wound
- Avoid any cream/ointment/powder to the wound
- If there are blue stitches sticking out from your incisional wound, they will be removed on your next clinic visit
2. Signs & symptoms of wound infection as follows:

Call your Thoracic Nurse or Case Manager (office hours 9am - 5pm) regarding surgical wound and pain management.
Name card will be provided.
3. Self recovery at home
Incisions
You may continue to experience itchiness or tingling sensations and pain in the chest around the incision area for about 6 months. It may take up to 1 year for the itchiness/tingling sensation to be reduced.
- Soreness and numbness may occuron your incisions, back and shoulders. In the first 4-6 weeks, changes in the weather, lying in one position too long or not getting enough exercise may cause you to feel more stiff and sore.
- Bruising (especially along the incisional wound), will fade and eventually disappear.
- The lump or swelling at the top of your incision will gradually reduce over the next 3 months.
- Sharp, shooting pains that lasts momentarily may take up to 6 months to disappear.
4. Medication adherence
- Take the pain medications as prescribed
- Make sure the medications can last till the next follow-up appointment
- Seek medical help if there are side effects such as rash, fever, vomiting, diarrhea, severe bruising etc.
5. Importance of early exercise and return to physical activity
- Your physiotherapist will provide you with a customized exercise after your surgery.
- You will be encouraged to start early mobility and adequate deep breathing exercises as required.
- Good posture is important for optimal wound healing and maintenance of range and strength.
- Regular walking with slow deep breathing exercises is essential to prevent complications after surgery.
- Avoid any heavy lifting for at least 1 month after surgery.
- Only resume your usual exercise after discussion with your doctor during your next clinic session.
6. Lifestyle and diet modification
- STOP smoking
- Resume a well-balanced diet as soon as possible
- Increased protein intake is encouraged