Revolutionising Critical Care
The Extracorporeal Membrance Oxygenation (ECMO) Journey
PULSE Issue 44 | January 2025
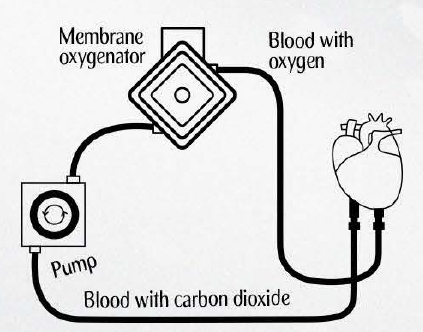
ECMO offers a lifeline for patients with severe cardiac or respiratory failure. Imagine a machine that temporarily takes over the function of the heart and lungs. This is precisely what ECMO does. Known in the medical community as Extracorporeal Life Support (ECLS), this specialised technology temporarily replaces the heart and lungs’ function by oxygenating blood and removing carbon dioxide through an external circuit.
Extracorporeal Membrane Oxygenation (ECMO) is often seen as an advanced, heroic form of life support, used to treat critically ill patients with refractory heart or lung failure, who would otherwise face certain death. Early use of ECMO did not show significant improvements in outcomes for those with cardiogenic shock1, leading many hospitals to pause its use. However, the Influenza A (H1N1) global pandemic in 2009 reignited interest and sparked a revolution in ECMO therapy. Meanwhile, neonatal and paediatric clinicians had already begun to harness its potential, successfully treating children with refractory lung or heart failure since a landmark neonatal case in 1975.
Acting as a short term artificial lung or heart, ECMO provides critical circulatory support, allowing patients time to recover, or as a bridge to a life-saving transplant.
Refining Usage of a Life-saving Technique
At the heart of this transformation is Dr Robert H. Bartlett, also known as the father of modern extracorporeal support. As a young resident at the Boston Children’s Hospital in the mid-1960s, he had observed first-hand the effectiveness of cardiopulmonary bypass in keeping patients alive, even when the heart was stopped for surgery and the lungs were deflated. Determined to bring this promising technology into the Intensive Care Unit (ICU), he devoted his career in pursuit of this goal. He continues to run an ECMO research laboratory in Michigan and remains a leading authority in the field, gracing many ECMO meetings while serving as an inspiration to his successors.
As ECMO became a mainstay of therapy for patients in North America, especially in infants with severe Persistent Pulmonary Hypertension of the Newborn (PPHN)2, Dr Bartlett set up an organisation where like-minded clinicians could maintain a data registry of their patients and discuss problems encountered. This culminated in the founding of the Extracorporeal Life Support Organization (ELSO) in 1989. Unlike most medical societies, ELSO encompasses a multidisciplinary team of diverse clinicians – including nurses, respiratory therapists, perfusionists, ICU physicians, surgeons, and neonatologists, who care for patients of all ages, from premature infants to octogenarians.
Singapore and NUHCS’ Roles in Shaping ELSO Progress
Since then, the ELSO Registry has rapidly grown to become the most important data source for scientific research on patients supported with ECMO. At present, there are over 230,000 patients in the Registry3, which is the single largest ECMO database in the world. Over 100,000 of these patients survived to hospital discharge. It is likely that most of them would have died without ECMO support.
ELSO is also the largest global, nonprofit medical society focused on extracorporeal life support, having grown from 15 member centres in 1989 to nearly 750 in 2024, including many of the world’s leading healthcare institutions.


A Life-saving Journey
Through the COVID-19 Pandemic In 2018, the Ministry of Health (MOH) in Singapore recognised ECMO’s crucial role in optimising outcomes for the critically ill, but highlighted the importance of providing appropriate recommendations on usage and patient selection for this resource intensive procedure. That same year, MOH established the National ECMO Services Advisory Workgroup, to set standards and protocols for its use, just before the onset of the COVID-19 pandemic.
This foresight proved invaluable, as healthcare teams scrambled to provide ECMO support for patients suffering from severe COVID-19- related respiratory failure. The committee has since evolved into the National ECMO Standing Committee, comprising representatives from every government-restructured hospital in Singapore. Together, they continuously assess ECMO services and patient outcomes. Meanwhile, the ELSO Registry provides important data to benchmark outcomes of ECMO support against that of similar patient profiles in the neighbouring Asia Pacific region and the rest of the globe.
Looking Ahead: The Future of ECMO
Gaining momentum over the past decades, ongoing research in ECMO is of vital importance to refine clinical practice, and move the field forward in critical care medicine. Fostered by Dr Bartlett and ELSO, the international ECMO community continues to advance interprofessional education, united by a shared desire to do everything possible for patients and their families.
NUHCS is proud to play a pivotal role in this collective effort, enhancing knowledge, refining skills, and nurturing the next generation of ECMO practitioners. The journey of ECMO is far from over, and the institute remains steadfast in its commitment to bettering outcomes and shaping healthier lives through cardiac critical care.
1. Cardiogenic Shock – a life-threatening condition where there is a sudden deteriorarion of heart function, resulting in a weakened heart and inability to pump sufficient blood around the body.
2. Severe Persistent Pulmonary Hypertension of the Newborn (PPHN) – a serious medical condition in which a newborn’s circulatory system does not adapt properly to life outside the womb, and can be life-threatening.
3. Information accurate as at December 2024 (www.elso.org).
