Minimally Invasive Cardiac Surgery Programme - National University Heart Centre, Singapore
Minimally Invasive denotes less trauma and burden to the patient. Otherwise known as “Keyhole”, Minimally Invasive Heart Surgery encompasses operations on the heart coronary arteries, heart rhythm and heart valves, that are performed without opening the chest bone (median sternotomy), or by not using the heart-lung machine, or stopping the heart (in certain situations). Hence, a more appropriate term for Minimally Invasive Heart Surgery may be “Less Invasive”, compared to the traditional way heart surgery has been carried out in the past decades.
Technology is evolving, surgical experience is growing, and with it, patients' and doctors’ expectations change. Nowadays, patients are more embedded in active life, more educated, and with technology’s progress in the era of the Internet and Information flow, they expect to survive, have a good and durable outcome, to go back to normal activities as fast as possible, and walk out with the smallest possible trauma and scar.
The operations that can be performed in minimally invasive fashion are:
- Minimally Invasive Bypass Surgery
- Hybrid Bypass Surgery
- Minimally Invasive Mitral Valve Surgery
- Minimally Invasive Aortic Valve Surgery
- Minimally Invasive Tricuspid Valve Surgery
- Minimally Invasive Closure of Atrial Septal Defects
- Minimally Invasive Arrhythmia Surgery (Atrial Ablation)
- Combinations thereof.
Table 1: The table below shows potential advantages and disadvantages of Minimally Invasive Heart Surgery.
Advantages
| Disadvantages
|
Less trauma and surgical burden
| Requires (as do open surgeries) special training and tools
|
Less pain (in some occasions)
| Slightly longer operation time |
Less scar or disfigurement/better cosmesis
| Smaller access
|
Faster recovery
| Some major and complex operations may not be possible
|
Less blood loss
| May need conversion to median sternotomy |
Less infections
| |
Less heart rate irregularities (arrhythmia)
| |
Faster return to work
| |
1. Mitral Valve Surgery
The mitral valve is one of the frequent and prime targets for Minimally Invasive Heart Surgery.
The mitral valve is situated in the left heart chamber, and separates the left atrium from the left heart chamber. When it leaks or is blocked, high pressure builds up in the left atrium, which usually dilates, resulting in secondary side-effects, such as high lung pressure and irregular heart rhythm (atrial fibrillation). The access for keyhole mitral valve surgery is through a small cut of about 5-6 cm on the right side of the chest. This incision provides good visibility and access to the mitral valve. It also allows for various other separate or concurrent procedures, such as the tricuspid valve surgery, arrhythmia surgery, closure of holes in the heart, and combinations thereof.
There are a few conditions of the mitral valve which can be addressed in this setup:
- Mitral valve stenosis
- Mitral valve leakage (regurgitation)
- Mitral Valve Endocarditis (heart valve infection)
- Left atrial tumors (myxoma and others)
- As well as concurrent conditions mentioned above.
This operation requires special equipment and setup and is one of our frequently sought-for domains. First, a mitral valve surgeon must be able to repair, rather than replace the mitral valve, before transitioning his practice to the minimally invasive approach.
2. Coronary Artery Bypass Surgery
Bypass surgery is performed frequently nowadays, both in men and women. Bypass surgery is meant for patients with clogged (coronary) arteries of the heart, where medications, ballooning or stenting cannot help anymore. Bypass surgery in advanced cases of heart artery disease can be the more promising solution to pursue. Bypass surgery in our times can be performed safely and efficiently, at very low risk, depending on every patient’s history and concurrent problems.
Bypass surgery can now be performed in less invasive ways, such as
- Off-Pump: without stopping the heart and without using the heart lung machine.
- On-Pump beating heart: using the heart lung machine but without stopping the heart.
- MIDCABG and MVST: through a small incision on the front-side surface of the chest, just below and left to the left nipple.
- Hybrid: the cardiologist and heart surgeon working together.
2.1. Off-Pump:
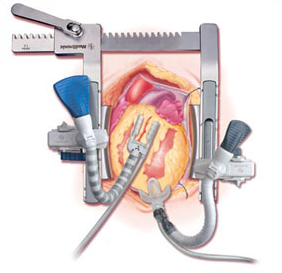
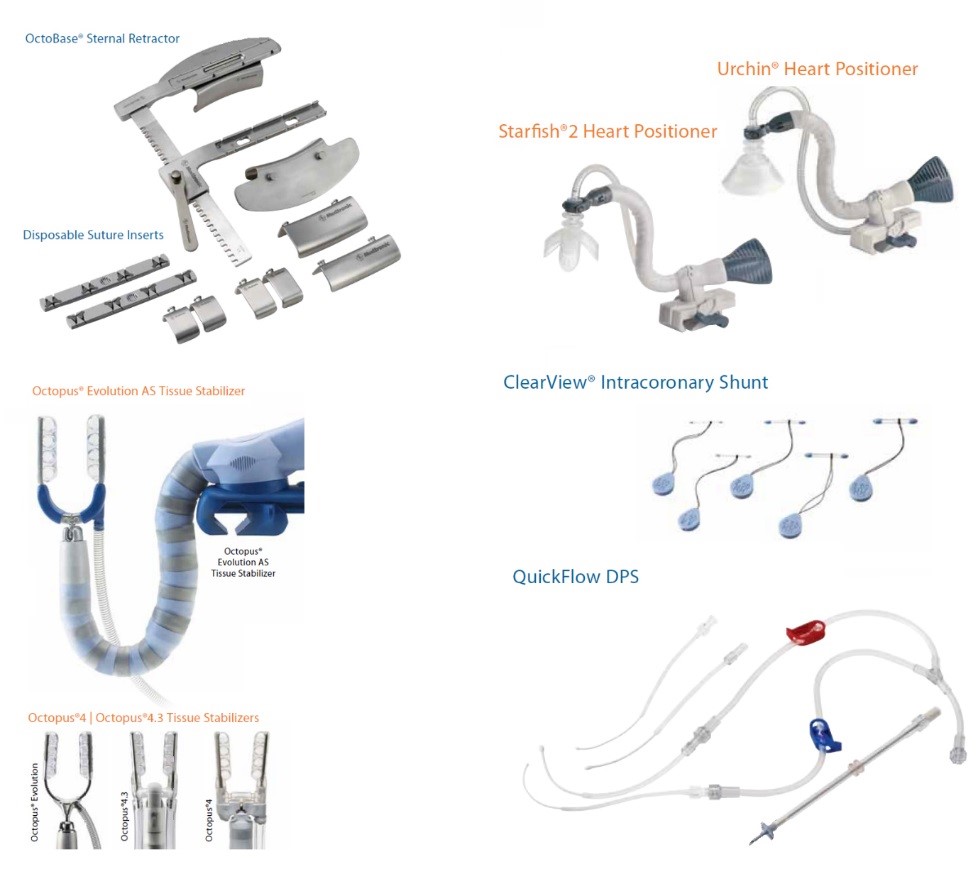
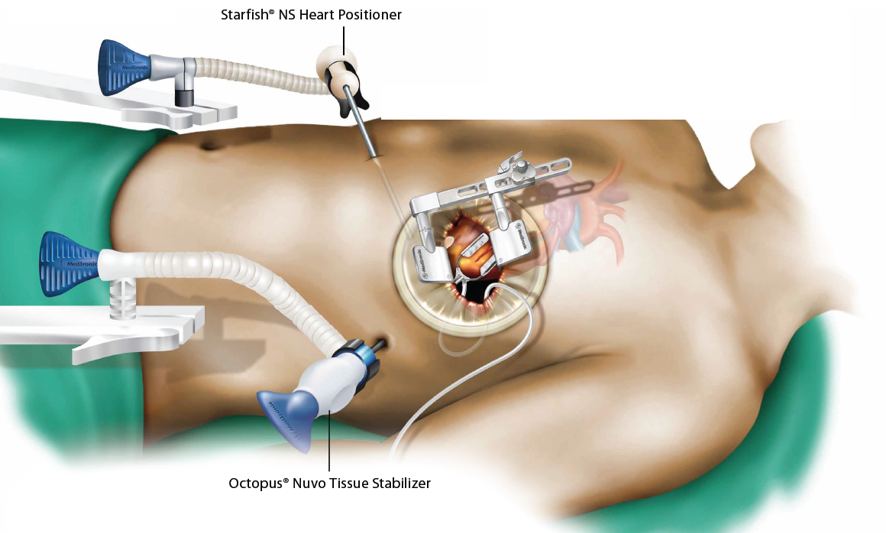
The entry is through a median sternotomy and the heart does not need to be stopped. The surgeon can maneuver and position the heart in a manner such that he is able to stitch the bypasses on the clogged vessels of the heart safely through the use of special equipment, including heart positioning devices (as seen in figure 3) and suction tools. Off-Pump surgery has been studied thoroughly and is slightly more beneficial in terms of stroke risk (if done without touching the aorta), loss of blood and need for transfusions, and overall length of stay in hospital.
| 
|
Figure 3: Heart Positioning Devices
2.2. On-Pump beating heart:
In some cases, the conditions of the patient do not allow for the surgeon to perform the bypass operation on a beating heart. Following are examples of such situations: The heart function is very bad, the arteries of the heart are very thin and calcified, or the heart surface is covered with fat tissue or adhesions. This bears the risk that he may abandon executing some of the initially planned bypasses, in case of “incomplete revascularisation”, or “incomplete bypass surgery”. Sometimes, it is very difficult to cover all planned arteries. In such cases, the surgeon may decide to connect the patient to the heart lung machine and empty the heart (without stopping it) to cater for more space, resulting in an easier job to carry out the bypass connections, without having to manipulate and squeeze the heart too much, while the patient remains stable.
2.3. MIDCABG and MVST:
This is one of the examples of Minimally Invasive Heart Surgery: stitch the bypasses through the side of the chest wall, without breaking any bone, just by going through the ribs. This procedure was first introduced in the 70s, but later abandoned because it was only meant for patients with one single blockage during those times. Since then, cardiologists have taken over and treat single-vessel-disease, making the procedure almost obsolete. It has however been revived, with the advancement of technology such that all three arteries of the heart can now be bypassed from the same small chest wall incision, under the nipple. Established and propagated by Professor Joe McGinn in New York, we have introduced this procedure since 2014. Many patients may qualify for this procedure, which can be used as a sole surgical option, or in combination with the cardiologist (hybrid procedure). For this type of minimally bypass procedure, a more extensive patient preparation may be required, in the form of a preoperative CT scan, to rule out severe disease of the aorta and peripheral arteries, a factor that would render the operation risky.
2.4. Hybrid Bypass Procedure
In some cases, the surgeon cannot place all necessary bypasses through the small chest wall incision. He will then suffice to stitch 2 out of 3 or 4 bypasses, and the procedure can be easily completed by the cardiologist later by inserting 1 or 2 stents. This provides full revascularization of the heart, as intended, while keeping the procedure ‘keyhole’. We are now able to perform this procedure in a single operation (both bypasses and stenting in one, “one stop”-hybrid bypass procedure). This is made possible due to our hybrid operation theatre and equipment, as well as a well-coordinated team of doctors and nurses. This procedure provides the heart with the missing blood and oxygen supply, but may cost slightly more (about 10-15% more than the conventional bypass procedure). The benefits of this procedure are much faster recovery and mobility of the patient, and other advantages such as less blood loss, less transfusions, less infections and better cosmesis.
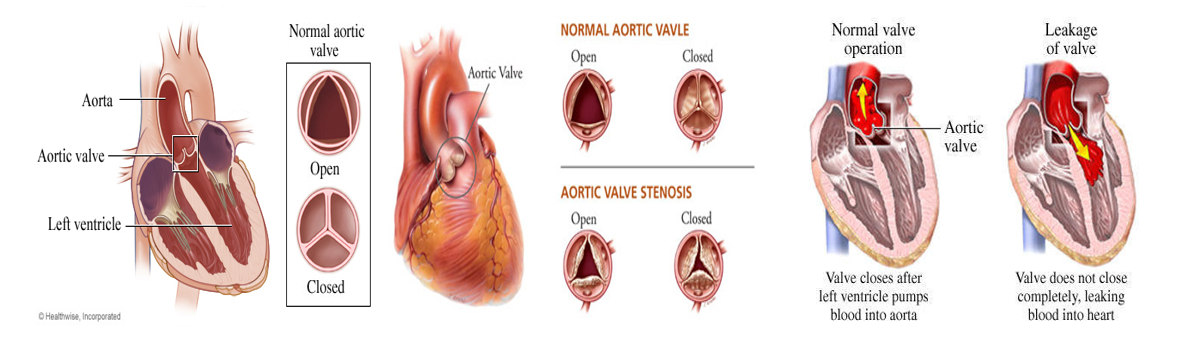
2.5. Aortic Valve Surgery
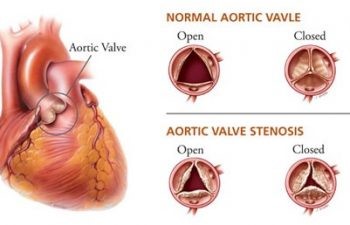
The aortic valve sits at the exit of the left heart chamber. The left heart chamber, at every heart beat, propels blood with high speed and pressure through the aortic valve into the aorta, the main vessels from the heart. Over the years, this valve can deteriorate as it is exposed to wear and tear, and can block (aortic valve stenosis). It can also leak, allowing a major portion of the blood to flow in the wrong direction, back into the heart chamber. In both cases, when the condition is advanced, the valve needs to be replaced. The traditional way this was done was through opening the chest bone. In our practice, every patient presented with such a condition will be considered for Minimally Invasive Aortic Valve Replacement.
This procedure can be done in two ways:
- Through a mini (partial) sternotomy
- Through a mini-thoracotomy, which is even less invasive.
The position and pathological conditions of the aortic valve:
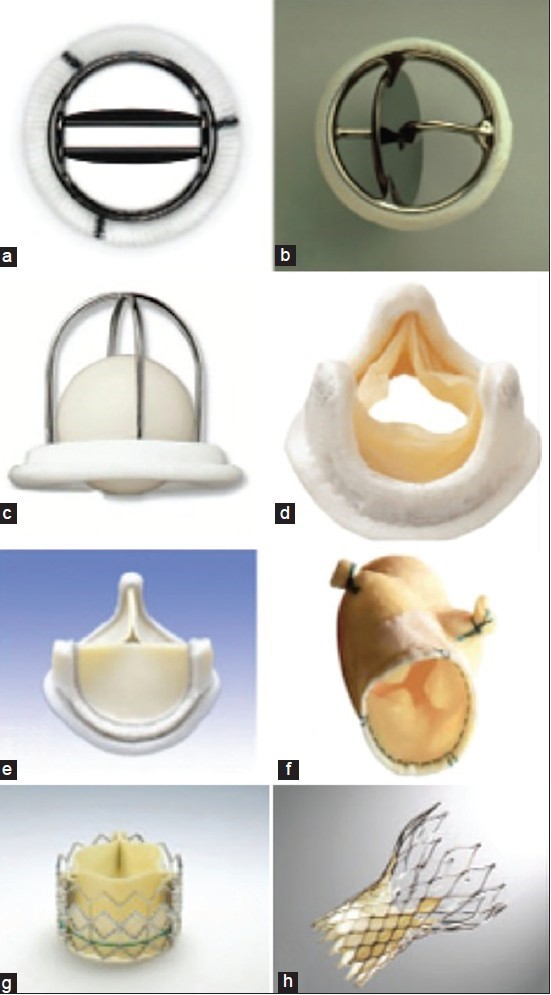
Some of the Aortic Valve prosthesis, which we use to replace the aortic valve: mechanical and biological prostheses:
The risk and degree of difficulty in replacing the aortic valve varies from patient to patient. In many cases, the patient presents with multiple medical conditions, such as stenosis of the aortic valve and blockages of the heart arteries, which also needs to be operated. Such instances of combined conditions may disqualify the patient for minimally invasive approaches, but this can be discussed and planned.
The procedure is relatively straight forward, given the appropriate tools and exposure. The first option entails only partial opening of the chest bone, which does not destabilise the chest cavity as much as median sternotomy does, usually allowing patients to recover faster. The procedure is also better cosmetically. The surgeon can obtain access to the heart and vessels of the same through a partial sternotomy. The aortic valve can be repaired or replaced, depending on the patient’s specific condition. In our practice, we have even operated emergencies, such as aortic tears, when indicated, through a partial mini sternotomy, as this incision allows for a good exposure of the upper portion of the aorta.
In the second approach, called “Mini-thoracotomy”, a 4-6 cm incision is fashioned between the second and third ribs, without touching the chest bone, around 3 cm to the side of it. However, patients must meet the conditions to qualify for it. Any singular aortic valve problem may be a good candidate for this procedure, except patients with disadvantageous anatomy – These are patients whose aorta is shifted far to the left of the chest bone, making the access from the front and right of the chest not optimal. Therefore, a CT scan is necessary and critical for every patient in question for this procedure. Once the qualifying criteria are met, patients can receive an aortic valve repair or replacement and return to full functionality earlier.
After the introduction of new devices in Asia, such as the sutureless aortic valves and automated knot-tying devices, Minimally Invasive Aortic Valve Surgery has become much easier.
2.6. Minimally Invasive Arrhythmia Surgery /Atrial Ablation
A large number of people suffer from irregular heart-rhythm or rate. In majority of the cases, this can be treated with medications. In some cases however, surgery is warranted. The most frequent form of arrhythmia is atrial fibrillation where the atria of the heart do not beat in synchrony with the chambers, thereby causing blood to flow slowly and turbulently in some areas. Clogs may form and cause a stroke in the patient. As such, many patients are placed on blood thinners. Atrial fibrillation also reduces the pump function of the heart causing symptoms of fatigue.
Some patients present with their main heart problem, which may be a leakage of the mitral valve, and atrial fibrillation at the same time. Some patients have an intractable, lone-standing atrial fibrillation as their main concern. In both cases, a method called atrial ablation can help.
In our program, we use mostly radiofrequency ablation, a method that applies radiofrequency-induced heat on the surface of the heart that conducts the irregular heart rhythm, and stops it. There is a >85% likelihood for this method to succeed in stopping the atrial fibrillation and bringing the patient’s heart back to its normal rhythm, when done properly.
Atrial ablation can be administered during open surgery and keyhole surgery, depending on the underlying condition. We prefer to use modern equipment, such as Pen-like devices to apply radiofrequency heat on the surface of the heart, both outside as well as inside. For the minimally invasive atrial ablation, which we have introduced, as a first in Asia, we use the “Cobra-Fusion” device, which magnetically finds its way around the heart, and applies radiofrequency with high precision through camera-holes.
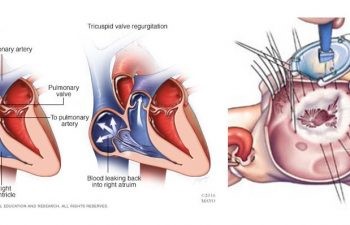
2.7. Minimally Invasive Tricuspid Valve Surgery
Many call the tricuspid valve the “forgotten valve” of the heart. It is rare that the tricuspid valve alone will cause any major health problems. However, it often leaks when other valves are diseased, or other heart conditions exist. A leakage of the tricuspid valve can cause serious symptoms and results in heart failure. Recognition and decisive treatment is key. Surgery of tricuspid valve is done usually through conventional open heart surgery, through the chest bone, and requires bi-caval cannulation (inserting two, instead of one cannulas in the right side of the heart) to run the heart lung machine.
However in our practice, we perform every single tricuspid valve surgery that comes as a stand-alone problem minimally invasively, and often without stopping the heart. Even if the tricuspid valve leakage occurs concurrent to other problems, such as mitral valve leakage, we will still prefer to operate these conditions through the minimally invasive route, rather than through opening the chest bone. Nowadays, we are operating three or four conditions of the heart at the same time, in the same keyhole session. In vast majority of cases, we aim and succeed in repairing the tricuspid valve, without replacing it.
2.8. VE ASD Closure
Some people are born with congenital heart defects. Some involve a hole between the two atria of the heart, the left and the right, and are called “Atrial Septal Defect”. In some occasions, the hole becomes so big, that it causes disadvantageous shifts of pressures within the heart, and may even result in a stroke. When indication is present, people, often in young age, will seek help for a keyhole closure of the ‘hole’ in their heart. This brief and minimal operation brings relief and safety to the patient and he/she will be able to return to normal activities within a few days.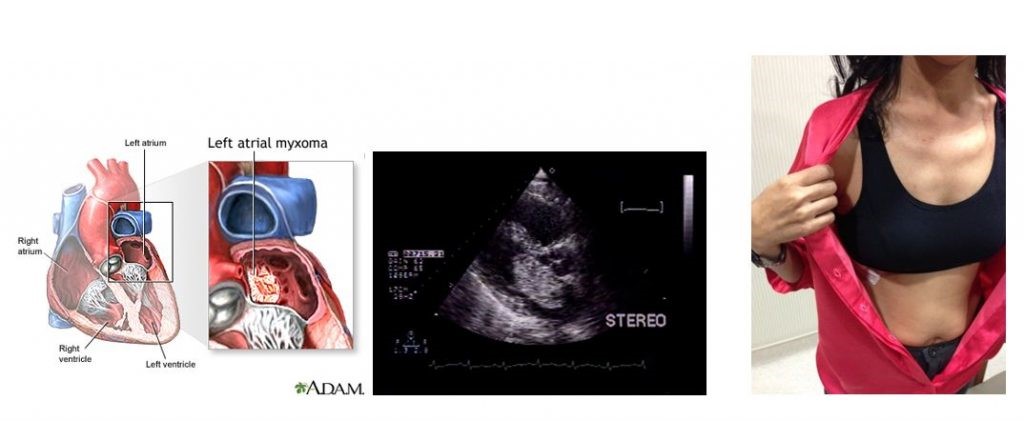
2.9. Minimally Invasive Heart Tumor Operations
Heart tumors are thankfully rare. One of the most frequent forms of heart tumor is the left atrial myxomas, and thrombosis of various origin. Some of them grow to a dangerous size, threatening to block blood flow or wash off in the blood stream, causing stroke or pulmonary embolism. In both cases, the operation can be done with a minimally invasive approach, except in some rare scenarios. The access is the same, through a small incision between the ribs on the right side of the chest.
2.10. Minimally Invasive Surgery for Combined Heart Operations
With the advancement of technology and skills, carrying out single-pathology operations are no longer the standard routine but rather multiple ones instead. We will continue to strive to minimise and further simplify operations for the benefit our patients.
Some of the common combinations of operations carried in a single setting are:
- Mitral Valve Surgery + Tricuspid Valve Surgery
- Mitral Valve Surgery and Atrial Ablation
- Mitral Valve Surgery and ASD closure Heart Tumor Removal and Bypass Surgery (First in Asia, done by ourselves)
- And others
2.11. Minimally Invasive Redo Procedures
If you had a heart operation before and need to undergo heart surgery a second time, you may qualify for Minimally Invasive Heart Surgery. In some occasions, such keyhole surgery may help lower the risk, and is more manageable for the patient. Prior to the second-time surgery, the patient may require a preoperative CT scan to study the current position of the heart in relation to the chest wall, and check on adhesions.