Acute coronary syndrome is an umbrella term for any condition brought on when blood flow to the heart muscle is reduced suddenly.
The doctor will take your medical history and give you a physical examination. If the doctor suspects an acute coronary syndrome, usually the following tests will be performed:
- Blood test
- An electrocardiogram (ECG) to determine the electrical activity of the heartbeats
Additional tests may be ordered by the doctor for further examination of the condition of your heart.
The symptoms are similar to that experienced during a heart attack. It is important to treat it as soon as possible. You should seek emergency help right away if you experience these symptoms and think you're having a heart attack.
- Chest pain
- Pain in the jaw or upper arm
- Shortness of breath
- Nausea/Vomiting
1. Electrocardiogram (ECG or EKG)
1.1. What is it?
An electrocardiogram (ECG or EKG) is a non-invasive test that measures the electrical activity of the heartbeats. An electrical impulse travels through the heart with each beat. This impulse causes the heart muscle to squeeze and pump blood. An electrocardiographic machine detects these impulses and records them in the form of waves.
This test allows the doctors to evaluate the regularity of the patient's heart rhythm or abnormality, if any.
1.2. Why is it done?
An ECG gives two major kinds of information. First, by measuring time intervals on the ECG, a doctor can determine how long the electrical wave takes to pass through the heart. Finding out how long a wave takes to travel from one part of the heart to the next shows if the electrical activity is normal or slow, fast or irregular. Second, by measuring the amount of electrical activity passing through the heart muscle, a cardiologist may be able to find out if parts of the heart are too large or are overworked.
1.3. Does it hurt?
No. There’s no pain or risk associated with having an electrocardiogram. When the ECG stickers are removed, there may be some minor discomfort.
2. Coronary Angiography
2.1. Overview

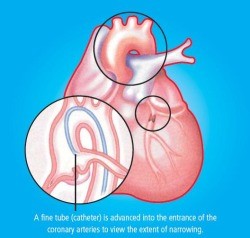
Coronary Angiography is a procedure to visualise the coronary arteries. The coronary arteries are the blood vessels that supply blood to the heart muscles. On ordinary chest X-ray films, the heart appears as a silhouette and the coronary arteries cannot be seen. To see the coronary arteries, a special dye or contrast medium is injected through a small tube (catheter) inserted into a large artery in the groin or the wrist. The catheter is then advanced to the heart and positioned at the mouths of the coronary arteries before injection is performed.
Coronary angiography is therefore an invasive procedure. Sometimes, another procedure called a left ventriculography is performed at the same session, whereby a catheter is advanced into the left ventricle (the lower and larger heart chamber) and contrast medium is injected. This allows visualisation of the left ventricle and its contractions.
2.2. What is the purpose of this test?
In some people, the coronary arteries become narrowed, usually by a process called atherosclerosis in which cholesterol and other substances are deposited in the arterial wall. With progressive narrowing, the blood supply to the heart muscle gradually decreases, and eventually becomes insufficient to supply its needs. This usually results in chest pain (angina pectoris) during exertion or stress, but may also manifest as breathlessness, irregular heart rhythm or fatigue. When a blood vessel suddenly occludes completely, a full-blown heart attack occurs. Coronary artery disease is a common disease and a major killer in Singapore.
Coronary Angiography is carried out to determine whether there is any significant narrowing or blockage in the coronary arteries. Once determined, the doctor will decide on the best form of treatment to carry out.
It is also performed before Coronary Angioplasty (ballooning) is carried out to provide a 'road map' for guiding the Angioplasty procedure.
2.3. What to expect?
The procedure may be performed on an outpatient basis, or you may be admitted overnight.
Before the procedure:
- Routine investigations, including blood tests, an Electrocardiogram (ECG) and a chest X-ray may be carried out.
- You would not be allowed food and water for 6-8 hours before the procedure.
- A small cannula will be inserted in one of the veins on your hand/arm to facilitate injection of medicine, if necessary.
- You would be asked to sign a consent form after your doctor has explained the risks of the procedure to you.
On the day of the procedure:
- On the morning of the test, you will be asked to empty your bladder, and skin shaving usually on your groins and upper thighs will be done.
- You will be brought to the Invasive Cardiac Laboratory where you will be placed on a movable table, with X-ray cameras and LCD monitors around you.
- Do not be alarmed by the sound of the machines and you should try to relax and keep still.
- A nurse will clean your groin or wrist, and then drape you with sterile towels.
- The cardiologist performing the procedure will first apply local anaesthetic on either area before the catheter is inserted into your body.
- The procedure is painless, except for the initial injection of local anaesthetic.
- If left ventriculography is performed, you will feel a warm sensation in your chest which then moves down to your legs during the injection of the contrast medium for a few seconds.
After the procedure:
- The procedure normally takes 15-30 minutes, following which the catheters will be removed.
- Upon removal, the doctor will discuss his findings with you.
- Your puncture site will be compressed for about 10 to 15 minutes until the bleeding stops and the compressive bandage will be applied.
- You would be brought back to your hospital bed where you would have to lie flat on your back for 4-6 hours until the doctor verifies that you are fit to walk.
- Your doctor will then discuss the findings of the angiography, as well as treatment options.
- You can be discharged in the evening on the same day or early next day.
2.4. What to prepare?
- Please inform your doctor of any allergy, in particular, allergies to seafood, iodine, X-ray contrast medium and pain relieving medications.
- Please inform your doctor if you have a history of peptic ulcer disease, recent strokes, or bleeding tendencies.
- If you are suffering from diabetes mellitus and you are taking a medication called metformin, please inform your doctor and you would need to stop this particular medication for at least 2 days before and after the Angiography.
- Bring along some light reading material or a mini radio for your hospital stay as you will be spending much of your time in bed.
- Please bring all your medications with you. You will be instructed on the medications that you will need to omit before the test.
2.5. What are the potential risks or complications?
Coronary Angiography is one of the safest invasive procedures. There is a small risk of injury and complications with regards to this procedure. Most complications are minor bleeding, swelling and bruising from the puncture site and allergic reaction from the contrast medium. There is a very small risk (0.1%) of heart attack and stroke occurring during the procedure, and an even smaller risk (less than 0.1%) of major life-threatening complications.
2.6. Home care
As a patient:
-
Resume normal daily activities.
-
Notify the doctor at once if you experience bleeding or increased bruising at the puncture site; or when you experience a recurrence of symptoms, such as breathlessness or decreased exercise tolerance.
Treatment for acute coronary syndrome varies. It ranges from medications to surgery methods to restore blood flow through your heart.
Medications can help to relieve chest pain and improve blood flow. Some medications your doctor could prescribe to you are aspirins, beta-blockers, cholesterol-lowering drugs etc. Procedures like angioplasty and stenting could also be recommended. Depending on the severity, the doctor could also recommend
coronary bypass surgery.
1. Coronary Angioplasty and Stenting
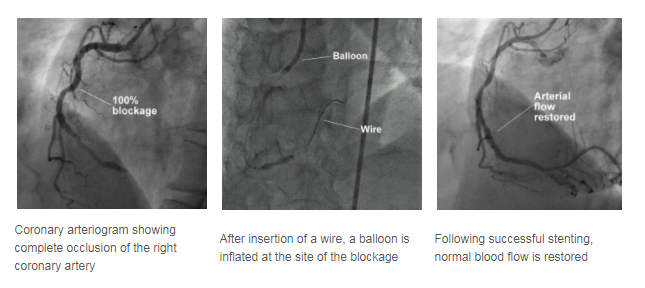
Coronary artery narrowings may be treated using either medications that reduce the heart's demand for blood, or by procedures aimed at increasing the heart's blood supply. One of the two most common methods to increase the blood supply is Coronary Angioplasty, sometimes abbreviated as PTCA (Percutaneous Transluminal Coronary Angioplasty).
PTCA offers a non-surgical alternative to Coronary Artery Bypass Surgery.
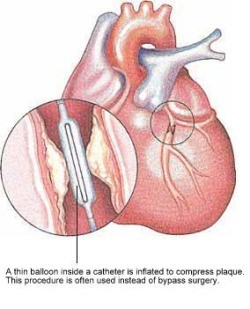
In PTCA, a balloon mounted on a thin tube (a catheter) is advanced into your coronary artery until it lies within the narrow area. The balloon is then inflated at high pressure, often a few times, to dilate the narrowing. Upon balloon deflation, the arterial narrowing is often significantly reduced.

A sample of a stent
A stent is a small metal coil to provide support to the narrowed segment of the coronary artery after angioplasty, preventing the artery from collapsing and reducing the likelihood of the narrowing recurring. Modern stents are made of stainless steel or a cobalt chromium alloy and are inert to the body. Some stents also have a medication coating and these may be preferred in certain situations to further reduce the chance of repeat narrowing of the heart arteries. Nowadays, stents are frequently placed directly over the narrowed segments (direct stenting) without prior balloon dilatation.
1.1. What to expect?
Before going through a PTCA, a coronary angiogram is done first to provide a 'roadmap'. Undergoing PTCA is also very similar to having a coronary angiogram procedure.
- First, you will be injected with local anaesthetic.
- A plastic tube known as sheath is inserted in a large artery in the groin or wrist. Through this sheath, a catheter is advanced to the mouth of the narrowed coronary artery.
- A thin wire is then threaded through the catheter and positioned in the coronary artery.
- Over this wire, the balloon catheter is pushed into the artery and the balloon positioned over the area of narrowing.
During balloon inflation, you may experience some chest discomfort, and you should report this to your attending cardiologist. Stenting is carried out in a similar manner. The procedure may take from 1 to 2 hours or more depending on the complexity of the diseased artery.
Following the successful PTCA, you will be monitored in a special monitoring ward. During this period, the sheath may be kept in your groin artery for 4 to 5 hours. However, the sheath may be removed immediately after the procedure if the situation allows. After the sheath is removed, the puncture site will be compressed for about 30 minutes to ensure that there is no bleeding.
You will have to remain in bed for several hours or until the following day to ensure the puncture site is sufficiently healed before walking. Your cardiologist will determine how long you need to stay in bed before you can walk around. Following that, some blood tests and ECGs will be performed to monitor your condition. If there are no complications, most patients can be discharged on the same day or the day after.
1.2. What to prepare?
- Please inform your doctor of any allergy, in particular, allergies to seafood, iodine, X-ray contrast medium and pain relieving medications.
- Please inform your doctor if you have a history of peptic ulcer disease, recent strokes, or blooding tendencies.
- If you are suffering from diabetes mellitus and you are taking a medication called metformin, please inform your doctor and you would need to stop this particular medication for at least 2 days before and after Angiography.
- After being discharged, you will be given two anti-blood clotting medications – aspirin and either ticlopidine or clopidogrel. For the latter two medicines (ticlopidine or clopidogrel), your cardiologist will advise you on the optimal length of time you should continue taking them. This can range from one month to one year. However, aspirin should be taken indefinitely to prevent future heart attacks, unless instructed otherwise by your cardiologist.
1.3. What are the success rates?
The success rate of Coronary Angioplasty is usually about 95%, depending on the nature of your coronary narrowing. However, in about 5% of cases, the procedure may be unsuccessful and the artery remains narrowed. In very few patients (about 1%), urgent bypass surgery may be required if the procedure is complicated.
There is a possibility of a recurrence of the narrowing of the coronary artery in the 6 months following the initial successful angioplasty or stenting, and you would usually feel a chest discomfort should it happen. If you feel a chest pain, you should seek medical attention immediately and inform your doctor.
1.4. What are the potential risks or complications?
Major complications like heart attacks, abnormal heart rhythm, stroke and death occur in less than 1% of the patients undergoing PTCA.
Less serious complications like bleeding from the puncture site, bruising and swelling of the puncture site, and blood clot formation in the artery where the sheath is inserted occur in 1-3% of the patients.
Overall, the procedure is very safe and well-tolerated.
1.5. Home Care
As a patient:
- Resume normal daily activities.
- Notify the doctor at once if you experience bleeding or increased bruising at the puncture site; or when you experience a recurrence of symptoms, such as breathlessness or decreased exercise tolerance.
- Comply with regular follow-up visits.
2. Coronary Artery Bypass Surgery
Coronary artery bypass surgery is an operation that is carried out to improve the flow of blood to the heart muscle in people with coronary heart disease where the coronary arteries are severely narrowed or blocked.
The operation involves taking blood vessels from other parts of the body and attaching them to the coronary arteries past the blockage. The blood is then able to flow around, or "bypass" the blockage. If more than one artery is blocked, you may need more than one bypass.
2.1. How should you prepare for the surgery?
- Stop smoking if you are a smoker. You should stop smoking because smoking is a risk factor for coronary heart disease. Your heart disease will not improve if you continue to smoke. It also increases your risk of complications from the surgery.
- Talk to your doctor or other people who have had the surgery. Knowing what to expect may help reduce your anxiety before the operation.
- Plan for your care and recovery after the operation. Allow for time to rest, and try to get help for your day-to-day activities.
2.2. What happens during the surgery?
- Coronary artery bypass surgery is performed by a team of surgeons.
- You will be under general anaesthesia throughout the procedure.
- The operation takes three to six hours, depending on how many blood vessels need to be bypassed.
- A cut is made in the center of the chest at the breastbone to allow the surgeon to see the heart.
- Another cut may be made in your leg to remove a vein that will be put in your chest. (In addition, an artery in the chest, called the internal mammary artery, can be used).
- If a vein is used for the bypass, one end of it is sewn into the aorta (the main artery from the heart to the body). The other end is sewn into the area beyond the blockage in the coronary artery.
- In the case of the mammary artery, the lower end of this artery is cut and attached to the coronary artery beyond the blockage.
- In either case, the blood will use the new vessels as a detour to bypass the blockage.
- Your chest will be closed with stitches at the end of the surgery.
2.3. What are the potential risks or complications?
- If you are healthy and under the age of 60, your risk of serious complications is 1%. If you are older, and especially if you are having chest pains, your risk of serious complications is 2% to 10%.
- There are always some risks when you have general anaesthesia. Discuss these risks with your doctor.
- There is a risk of infection or bleeding from this operation.
- New blockages can develop in the bypassed vessels. This might require another heart catheterisation and surgery. It is important to make changes to your lifestyle to decrease the risk of blockage.
- There is a risk of stroke during and after the operation.
2.4. What happens after the surgery?
- You will go to the intensive care unit (ICU) where you will stay for several days or as long as you need for observation. An electrocardiogram (ECG) monitor will record the rhythm of your heart continuously.
- You will have respiratory therapy to prevent any lung problems, such as a collapsed lung, infection, or pneumonia. A nurse or therapist will assess you with breathing exercises every few hours. Ask for pain medication if you need it.
- You will have physical therapy, which includes walking around the hospital and other strengthening activities. You will learn how to move your upper arms without hurting your breastbone.
- You will learn how to live a healthy lifestyle, such as choosing foods that are low in fat, cholesterol and salt, exercising regularly and not smoking.
2.5. Home care
- Have a relative or friend to pick you up on the day of your discharge.
- You will not need nursing at home, but it will be good to have someone help you with your shopping and also to support you for the first 10 days or so.
- Follow up with the pre-arranged check up at the hospital with your doctor.
- Full recovery should take about 3 months.
2.6. When should you call the doctor?
Call the doctor right away if:
- You develop a fever.
- You become short of breath.
- You have chest pain that becomes worse despite taking painkillers.
Call the doctor during office hours if:
- You have questions about the operation or its result.
- You want to make another appointment.