Paediatric Cardiac Surgery - National University Heart Centre, Singapore
Congenital means inborn or existing at birth.
Congenital heart disease (CHD) is the most common birth defect affecting approximately 1 neonate in every 120-166 births. About two-thirds of the patients need cardiac surgery in their lifetime; and half of the surgeries are required within the first six months of life. Congenital cardiac surgery is reconstructive surgery that aims for re-storing biventricular circulation, when possible. Single-stage primary complete repair has become the central philosophy since the 1980s. In about thirty percent, physiologic and anatomical reasons do not permit repair by a single operation; these patients endure staged-repairs and another 15% of CHD patients previously undergone cardiac surgery will require subsequent re-operations – mostly re-replacements of non-growing and/or deranged prostheses. Contemporary mortality rate of congenital cardiac surgery for neonates, infants, and children is reported between lower limit of 0,1% (repair of subvalvar aortic stenosis) and upper limit of 13.2% (Nor-wood-procedure) that places this human endeavour in the risk-range. Especially, neonates undergoing complex open-heart procedures with acuity are at high short-term risk. Owing to advanced treatment possibilities, CHD survival to adulthood now reaches 90-95% in developed countries from less than 20% in the presurgical era. Treating CHD patients has significant public health aspects and is a commitment for life.
Congenital heart disease or defect (CHD) is an abnormality of the structure of the heart that exists at birth. It occurs when the heart or major blood vessels fail to develop or mature normally during the pregnancy.
Terminology:
The list below describes some terms commonly used in CHD:
- Stenosis – Narrowing
- Atresia – Absence of connection between heart chambers or to great arteries that normally communicate
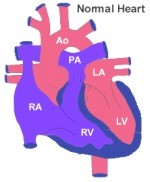
- Atrium and Ventricle - There are 4 chambers in the heart; both right and left having two each. The receiving chamber is called an atrium while the blood pumping chamber is called the ventricle. The heart also has four valves that prevent blood flow from leaking backwards.
- Mitral valve – This is the opening between the left atrium and left ventricle in the left side of the heart
- Tricuspid valve – This is the opening between the right atrium and right ventricle in the right side of the heart
- Aortic valve – This is the opening that connects the left ventricle of the heart with the aorta, which is the major blood vessel that delivers oxygenated blood to the body
- Pulmonary valve – The valve in the opening the connects the right ventricle to the vessels that deliver the used, oxygen depleted blood to the lungs
- Septum – The wall that divides the right and left sides of the heart; the wall that divides both the atria is called the atrial septum and the wall that divides both the ventricles is called the ventricular septum
- The circulation consists of two circuits in series. The left ventricle pumps out oxygenated blood into the body that reach out to the organs, e.g., brain, liver, kidneys, muscles and bowels, etc. Organs take up oxygen and nutrients from the blood flow that is returned to the heart's right atrium via the veins. Next the right ventricle pumps de-oxygenated blood into the pulmonary circuit where blood is replenished with oxygen. Oxygenated blood returns to the left atrium and the circulation starts all over again.
There are many different types of CHD that fall into four common categories of congenital defects.
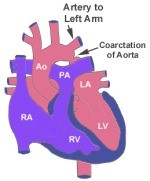
1. Obstruction to blood flow
This occurs when either abnormally formed heart valves or major blood vessels restrict or block the flow of blood into or out of the heart such as:
- Congenital aortic stenosis
- Mitral valve stenosis
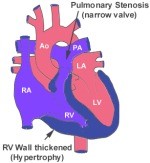
- Pulmonary valve atresia/stenosis
- Tetralogy of Fallot in which blood flow towards the lungs is obstructed
- Coarctation of aorta
- Interrupted aortic arch
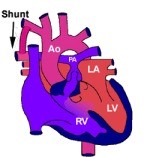
2. Left to right shunts
In a normal heart, the left and right sided heart chambers are kept separated.
However, in left to right shunt types of CHD, the blood flows from left side of heart into right side of heart. This is due to abnormal connection between right and left side of the heart. This results in the right side becoming overloaded with “extra volume” of blood. When this happens, it results in too much blood flowing into the lungs.
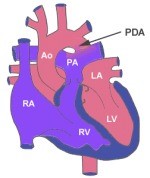
- Patent ductus arteriosus (PDA)
- Septal defects such as:
- Atrial septal defect (ASD)
- Ventricular septal defect (VSD)
- Atrio-Ventricular defect ( AVSD )
- Aorto-pulmonary window
3. Right to left shunts
In right to left shunts, the blood now flows from the right side of the heart to the left. This is also due to abnormal connection between the right and left side of the heart. It manifests in a decreased flow of blood into the lungs, which means that less blood is being oxygenated by the lungs. This condition is also called “cyanotic heart disease” as this condition causes a bluish colour of the skin (usually in the tip of fingers and toes) and mucous membranes (lips) due to the low oxygen levels in the blood.
- Tetralogy of Fallot (TOF)
- TOF has 4 abnormalities which are:
- VSD
- Over-riding of the aorta
- Pulmonary stenosis
- Right ventricular hypertrophy
- Pulmonary atresia with intact ventricular septum
- Pulmonary atresia with VSD
- Tricuspid atresia
- Ebstein's anomaly
4. Complex defects
These defects have more than one defect and are also known as “mixing defects”. They can present with cyanosis and also with imparied systemic circulation.
- Double outlet right ventricle (Tetralogy of Fallot type)
- Univentricular heart
- Total anomalous pulmonary venous connection
- Truncus arteriosus
- Hypoplastic left heart syndrome
- Transposition of Great Arteries ( TGA )
Medical and surgical treatments now offer these children an opportunity to grow and mature into adult life, an option that once was not available in the past.
How is it diagnosed?
Accurate diagnosis is necessary for the doctor to give appropriate treatment.
- Antenatal (before a child is born) diagnosis when a fetal cardiologist detects CHD during regular check-ups before the child is born
- If this is the case, plan of management and appropriate treatment can be fully discussed and planned with the parents before labour
- After the child is born when diagnosis is made soon after birth due to abnormalities detected in routine tests e.g.
- Abnormal (or low) oxygen saturation measurements
- Presence of heart murmurs during physical examination
- Severe symptoms of impaired circulation
- Other defects may only be diagnosed later on in the child's life.
Common tests used for diagnosis of CHD:
- Physical examination
- Electrocardiogram (ECG)
- 2-D echocardiogram (ECHO) - Gold Standard of Imaging
- Cardiac catheterisation
- Computer tomography, CT-angiography
- Cardiac magnetic resonance imaging (CMRI)
How does it affect my child’s health?
The presenting features of CHD depend on the age of your child and the type of defect present.
Common presenting features include:
- Failure to thrive (inability to grow) in small infants/ newborns
- Cyanosis
- Generalised duskiness in mild form
- Blueness in nail-beds/lips in severe form
- Decrease in exercise tolerance
- Breathlessness/dizziness/fainting episodes
- In servere situations: cardiogenic shock
If the condition is not corrected in a timely manner, damage to the heart and/or lungs could get beyond repair and consequently limit the life span of your child. Neonates with complex anomalies require urgent attention and treatment as haemodynamic situation can affect other organs, e.g. brain, kidneys, liver, etc.
In some cases, CHD may be life-threatening and must be surgically corrected:
- Hours after birth e.g. in total anomalous pulmonary venous drainage
- Within a few days e.g. in transposition of great arteries
In other cases, the operation can be carried out after a few months or years, whilst at times it is to repair the defect(s) in stages. Staged operations typically involve a lifesaving procedure as a neonate, for example, implanting a plastic tube to redirect the blood towards the lungs (i.e. systemopulmonary shunt) so that your child can grow bigger and stronger before carrying out a definitive procedure - e.g. In Tetralogy of Fallot.
Surgery for paediatric congenital heart diseases
1. Open heart surgery
- The chest cavity and the heart need to be opened in order to repair the defect.
- Most defects are inside the heart, so the surgeon opens the heart itself. In order to perform open-heart operations safely, a heart-lung machine ("cardiopulmonary bypass (CPB)") is connected to the patient's vessels. During the surgery, the machine oxygenates and circulates the blood.
Examples of conditions requiring open heart surgery:
1.2. Defects causing obstruction to blood flow
1.2.1. Pulmonary stenosis: The surgeon opens the narrowed valve
| 
|
1.2.2. Aortic stenosis: The surgeon opens the abnormal valve
1.2.3. Tetrology of Fallot (TOF): The surgeon opens the outlet towards the lungs and seperates the two ventricles
1.3. Defects involving the great arteries
Transposition of the great arteries
1.3.1. Surgery : Arterial Switch Operation: The surgeon restores normal connection of the left ventricle and aorta; right ventricle to the pulmonary artery; coronary arteries are reimplanted into the neo-aorta
1.4. Other complex defects
Hypoplastic left heart syndrome
1.4.1. Surgery : Norwood Stage I Surgery: The first stage operation involves arch repair, adequate inflow to the heart and contolled flow in the lungs. The Fontan operation creates a single circuit, where the only ventricle pumps out into the body and big veins connect directly into lung vessels.
2. Closed heart surgery
In this type of surgery the CPB machine is not used and the heart is visualised without having the heart opened.
Examples of conditions requiring closed heart surgery:
2.1. Patent ductus arteriosus (PDA): The surgeon closes the abnormal connection
2.1.2. Coarctation of aorta: The surgeon excises the narrowing of the aorta and restores normal blood flow towards the lower body
| 
|
How do I prepare my child for surgery?
- Your paediatric cardiologist will refer you and your child to a paediatric cardiac surgeon who will discuss with you the planned surgical procedure.
- Depending on the urgency of the surgery, the discussion will either take place in an out-patient clinic or in the ward.
- Once the date for surgery is fixed, your child will be admitted a day prior to the planned procedure for pre-operative preparation such as:
- Taking blood for routine tests
- Chest X-ray
- ECG
- The tests rule out any active infection or any other minor conditions that were not detected in previous investigations.
- As a parent, you would need to prepare yourself psychologically. Discuss with your child’s surgeon of any concerns that you may have.
- Should you prefer, you can request for a tour of the paediatrics intensive care unit to be arranged prior to surgery.
What happens during the surgery?
- You will be allowed to accompany your child into the area in the operating theatre where the anaesthetic doctor will prepare your child to receive general anaesthesia.
You child will be injected with or inhale in an anaesthetic agent to put him/her to sleep.
Once your child falls asleep, you will be asked to leave the operating theatre.
The anaesthetist will then insert a breathing tube (endotracheal tube) and put in various drips – central venous cathether, arterial cannula, intravenous cannula.
The time taken for the surgery would depend on the complexity of the procedure. It could between an hour to as long as 6 hours.
Once the procedure is successfully performed, you will be notified by one of the health professionals.
The surgeon will usually speak to you after the operation.
What are the potential risks or complications?
- The surgical team (paediatric cardiac surgeon and anaesthetist) will discuss the surgery in length with you. This includes the possible risks and benefits of the surgery.
- If surgery has been recommended for your child, this means that the doctors have good reason to believe that the benefits of the surgical intervention outweigh its risks.
- The major risks include:
- Risk to life
- Neurological abnormality
- Arrhythmia (irregular heartbeat) that may sometimes require insertion of a permanent pacemaker
- Abnormality of the kidney function that may require temporary dialysis and very rarely permanent dialysis
- Bleeding during or after the surgery
- Infection of the wounds
As a parent, you will be well informed of the risks and benefits of the surgery in advance so that you can make decisions with the help of the doctors.
What happens after the surgery?
- Your child will be transferred to the paediatric intensive care unit (PICU) after the operation.
- There will be many tubes connected to your child for various purposes, so don’t be alarmed.
- Your child will be usually be under deep sedation (asleep) usually up to 24 hours or sometimes long after surgery depending on the complexity of the surgery and age of the child.
- It is important to cooperate with the paediatric ICU staff who are well trained, caring and friendly.
- Usually a nurse will be assigned to solely look after your child during his/ her stay in ICU.
- As every patient is different, the staff will discuss your child’s hourly/ daily progress and treatment plans.
- Your child may be treated in the ICU for about 2 days depending on his/her recovery progress.
- When your child is stable, he/ she will then be transferred to a high dependency unit (HDU) for further close monitoring for another 1-2 days until he/she is stable enough to be transferred to the general paediatric ward.
- At this stage, most of the tubes and drips will be removed.
- Most of the recovery will be taken place in the general ward. Sometimes patients recover quickly and can go home from HDU.
- He/ she will be encouraged to move about and will be guided by a physiotherapist.
- Depending on the recovery progress, you can expect a period of 5-7 days in the general ward before your child is discharged from the hospital.
- A thorough physical examination and various investigations will be carried out prior to discharge. These tests are:
- Blood Tests
- ECG
- Chest X-ray
- 2-D ECHO
- During your child’s recovery period, parents are encouraged to get as much experience as possible. Once the child is discharged from the hospital, you will be solely looking after the child at home. This can be physically demanding and mentally challenging.
Home care
- After discharge, your child will be required to see both the cardiologist and the surgeon for review.
- At the first review, which is within two weeks of the discharge, your child will be examined thoroughly including a wound review and his/her medications will be reviewed and may be changed depending of how he/she is doing.
- For good cosmetic results, absorbable stitches are usually used for the large wounds. However, for the smaller wounds (e.g. the site where the chest drains were inserted after the surgery), non-absorbable sutures are used and these will be removed during the first review.
- Your child will then receive follow-up reviews by a paediatric cardiologist at regular intervals (usually 2 weeks, 6 weeks, 3 months, 6 months, 12 months and annually after discharge from the hospital) and necessary investigations will be carried out during these appointments.
When should you call the doctor?
Prior to your child’s discharge, he/she should be:
- Pain free
- Walking/running around per his/ her age
- Eating and drinking well
- Good bowel Movements
Rarely, the surgical wound may get infected after discharge from the hospital.
You should contact the ward/doctors/nursing staffs to make an appointment for an earlier review if you:
- Notice any ooze or redness from the surgical wound
- Have concerns regarding your child’s recovery at home
The review can be arranged as soon as possible so that you can be reassured and any potential problems picked up well in advance.
A/Prof Laszlo Kiraly
Head of Division & Senior Consultant, Department of Cardiac, Thoracic and Vascular Surgery
National University Heart Centre, Singapore
Asst Prof Winn Maung Maung Aye
Consultant, Department of Cardiac, Thoracic and Vascular Surgery
National University Heart Centre, Singapore
Dr Senthil Kumar Subbian
Consultant, Department of Cardiac, Thoracic and Vascular Surgery
National University Heart Centre, Singapore